Abstract
Social prescribing is a health policy initiative that aims to create closer links between health services and community activities. Despite its rapid adoption there are concerns about efficacy and value for money. We used a WELLBY (Wellbeing Adjusted Life Year) approach to identify the social value created through a national mental health-focussed green social prescribing (GSP) programme in England (2021-23). We found that GSP can lead to significant wellbeing benefits for people experiencing mental ill-health, with a social return on investment (SROI) of between £2.38-£5.90. However, we argue that the WELLBY approach should not be used uncritically. In our study WELLBYs proved to be an effective social value measure for low to mid cost GSP pathways where the target beneficiaries are likely to have mild to moderate mental health needs. For higher cost pathways providing targeted support for people with severe mental health needs the WELLBY was less effective and clinical measures of value may be more appropriate.
Introduction
Social prescribing is health policy initiative where systems, processes and pathways that connect health services and individuals with community-based activities are developed and implemented (Muhl et al., 2023). Social prescribing initiatives utilise the strengths of the local voluntary, community and social enterprise (VCSE) sector and are usually designed to address the social determinants of physical and mental health including wellbeing, social isolation and loneliness and community cohesion (Polley et al., 2019; Husk et al., 2020). However, when health systems invest in social prescribing commissioners also want to know whether it leads to reductions in costly healthcare interventions, and this question tends to dominate debates about whether or not social prescribing should be considered ‘good’ value for money (O’Connell Francischetto, 2024). This emphasis on measuring value to the health system is, we argue, ontologically dissonant with core principles of social prescribing, which prioritises creating value for individuals through a tailored conversation about ‘what matters to you?’(NHS, 2019).
Our research explores how the individual or social value of social prescribing initiatives can be measure more effectively and consistently. We used the WELLBY approach – Wellbeing Adjusted Life Year (see Frijters et al., 2024) – to value the wellbeing benefits for individuals in England who participated in the Tackling and Preventing Mental Ill-health Through Green Social Prescribing Project (GSP project). The article builds on our earlier GSP evaluation report which focussed on the value for money of the whole GSP programme, including national and local programmatic costs (see Haywood et al., 2024). Rather than restate the findings, the intention with this article is to elucidate the social value of green social prescribing (GSP) in a way that may be more useful to commissioners looking to develop similar initiatives outside of a national programme.
The article has three aims. First, to present an original methodology for applying the WELLBY approach to social prescribing, using the GSP project as a case study. Second, to articulate the results of applying WELLBYs to social prescribing, through an in-depth exploration of the costs and wellbeing benefits associated with a full GSP pathway. Third, to provide some critical reflections on the strengths and limitations of applying the WELLBY approach to social prescribing and to consider how and which contexts it could be applied more widely.
Although our data are drawn from a study undertaken in England focussing on nature-based social prescribing referrals it has broader relevance because our methodology is transferrable to other similar settings. It could be applied to other types of prescribed activities, such as creative or physical activities, and it could also be applied in other countries to understand the social value of different social prescribing models operating within other health system contexts. If our approach is widely adopted, it will enable greater consistency and comparability in research to understand the social value of social prescribing.
What are social prescribing and green social prescribing?
The term social prescribing describes systems, processes and pathways which enable practitioners within healthcare settings to connect their patients with non-medical support, typically at a community or neighbourhood level. Reflecting the global nature of social prescribing, and to help provide some consistency between different contextual understandings of social prescribing, a recent study used the Delphi method (Beiderbeck et al., 2021) to establish internationally accepted conceptual and operational definitions of social prescribing. The short conceptual definition says that social prescribing is:
a means for trusted individuals in clinical and community settings to identify that a person has non-medical, health-related social needs and to subsequently connect them to non-clinical supports and services within the community by co-producing a social prescription – a non-medical prescription, to improve health and well-being and to strengthen community connections (Muhl et al., 2023, p. 9).
Operationally, the definition describes social prescribing as ‘a holistic, person-centred and community-based approach to health and well-being that bridges the gap between clinical and non-clinical supports and services’ which requires an ‘identifier’ – such as a link worker – to identify an individual’s unmet non-medical, health-related social need and make an onward referral to activities and services (Muhl et al., 2023, p. 9). Although not explicit in this definition, many social prescribing initiatives also accept self-referral, whereby an individual accesses an activity without direct engagement with an ‘identifier’, if it relates to an unmet non-medical need (Haywood et al, 2024).
Primary care-based social prescribing in England, where this study was undertaken, involves a link worker who takes referrals from healthcare professionals – usually the GP – and starts with a ‘what matters to you’ conversation to understand the individual’s needs and preferences (NHS, 2019). The link worker then makes an onward referral to the activities and services, typically provided by the VCSE sector (Husk & Sanderson, 2024). Referral activities tend to fall into four broad categories: creative activities linked to art, culture or heritage; physical activities; activities in nature; or information, advice and guidance in relation to issues such as housing, finances and domestic violence. Building on this primary care model, there are examples of social prescribing being expanded into other clinical settings, such as mental health services (Dayson et al., 2020), and targeting specific populations, such as children and young people (Hayes et al., 2024).
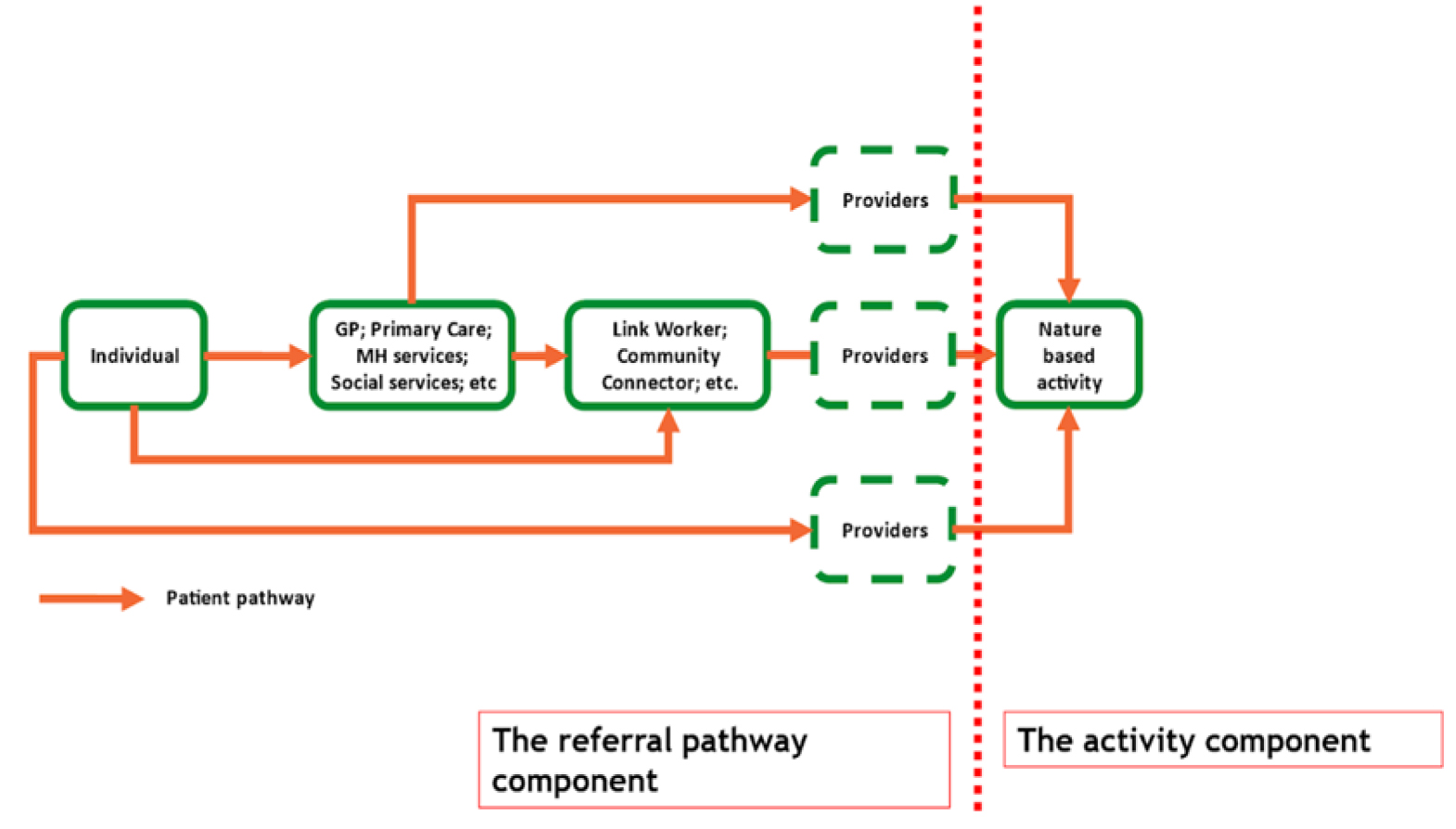
Green Social Prescribing (GSP), also known as nature-based social prescribing (NBSP), describes social prescribing referrals that involve individuals being encouraged to engage in activities in nature, often delivered by nature-based VCSE providers (De Bell et al., 2024). There are many different types of nature-based activities and therapies that people may reach through a social prescription. These include conservation and other hands-on practical environmental activities; horticulture and gardening; care farming; walking and other exercise groups in nature; and more formal talking therapies based in the outdoors (Fullam et al., 2021). Although the boundaries of GSP can be blurry, it is generally accepted that there are two key components to the pathway, a) the referral pathway and b) the activities to which people are referred (Figure 1). As Figure 1 shows, there is not a singular GSP pathway, as people may access nature-based activities via a number of routes including referral from a link worker (the centre line on the diagram), direct referral from a healthcare professional (the top line) or self-referral (the bottom line).
Figure 1: A simplified GSP pathway with the two key components highlighted
Reflecting growing policy interest in GSP, in 2021 the UK Government launched the England wide Preventing and Tackling Mental Ill Health through Green Social Prescribing Project (henceforth referred to as the GSP Project), a two-year £5.77m cross-governmental initiative focusing on how nature-based settings and activities to promote wellbeing and improve mental health can be embedded within healthcare systems at a local level (see Haywood et al., 2024 for more details). Funding was provided through HM Treasury’s Shared Outcomes Fund which supported pilot projects to test innovative ways of working across the public sector. The GSP project was centred on seven ‘Test and Learn’ sites (GSP sites) across England that explored how to make better use of green social prescribing to improve mental health outcomes; reduce health inequalities; reduce demand on the health and social care system; and develop best practice in making nature-based VCSE activities more resilient and accessible.
Social prescribing and the measurement of value
In evaluation, value for money (VFM) refers to a judgement about the optimal use of public or charitable resources associated with an investment and its stated aims and objectives (HM Treasury, 2021). Previous studies into the value of social prescribing have been based around two broad approaches: understanding the benefits to the health system through reductions in health service utilisation (O’Connell Francischetto, 2024) and exploring a wider range of social benefits drawing on the principles of social return on investment (SROI) (Canadian Red Cross, 2024; Foster et al., 2021). Both approaches have tended to yield largely positive results but also have some major limitations (Polley et al., 2019; Arvidson et al., 2013), as summarised below.
Studies exploring benefits to the health system tend to be relatively small scale and focussed on social prescribing services commissioned at the local level. In a review of such studies O’Connell Francischetto (2024) identified evaluations carried out in nine local health systems across England that found that social prescribing can substantially reduce pressure on the NHS, including through reduced GP appointments, reduced hospital admissions and reduced A&E visits. Due to their size and scale, these studies varied in methodological approach and quality and are limited by data availability, with some evaluations only having access to service user data, making control group analysis problematic (O’Connell Francischetto, 2024). A further limitation of these approaches is highlighted by the work of Polley et al. (2019), who identified more than 50 different outcomes that had been linked to social prescribing in previous studies. Broadly, these outcomes fell into three categories: the social determinants of health; health, including mental health; and health system utilisation (2019). This suggests that focussing solely on benefits to the health system risks missing a wider range of individual and societal outcomes.
With exception of two national SROI studies in Canada (Canadian Red Cross, 2024) and the UK (Foster et al., 2021) studies exploring social benefits have also tended to be small and local in terms of their scale. The Canadian study found that social prescribing delivers a return of $4.43 for every dollar invested, with benefits identified across a range of outcomes including hospital admissions, emergency visits, ambulance calls, loneliness and mental health (Canadian Red Cross, 2024). The UK study estimated a SROI of £3.42 per £1 invested, with benefits derived from improvements in service-users’ wellbeing valued at £5,426 per user (Foster et al., 2021). Although this second study has similarities with ours, different scales were used to measure wellbeing. Foster et al. (2021) used the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) whereas we used the Office for National Statistics (ONS) life satisfaction measure (part of what is known as the ONS4). Although both measures are endorsed by HM Treasury for measuring wellbeing, for studies taking a WELLBY approach the ONS measure is preferred and offers greater scope for replicability between studies (HM Treasury, 2021).
A number of local UK based studies have also identified positive SROI associated with social prescribing services, largely deriving from a combination of wellbeing benefits, wider community benefits and benefits for health systems (see Dayson & Bashir, 2014; Bertotti et al., 2020; Kimberlee, 2016). Although these studies have been helpful for the development of local level business cases for investment into social prescribing their local focus means they are less useful for national policy development. Further limitations include the lack of standardised methods and an absence of controlled studies. Although there are some commonalities between each study, they use different outcome metrics and take a variety of approaches to valuing benefits. This makes comparison and the aggregation of data from different studies very difficult (Arvidson et al., 2013). There is also no published evidence of the benefits associated with social prescribing being compared with alternative options or a ‘business as usual scenario’.
An alternative to the two approaches described above is the WELLBY, which uses a nationally standardised methodology for measuring and valuing wellbeing outcomes. Its main strengths in relation to social prescribing are twofold. First, it is endorsed by HM Treasury in its guidance for economic appraisal and evaluation (HM Treasury, 2021), giving the findings credibility and utility for national policy making. Second, studies consistently identify individual wellbeing as one of the main outcomes of social prescribing interventions (Polley et al., 2019), making WELLBYs a relevant and appropriate measure of value. The evaluation of the GSP Project presented an opportunity to explore the utility of the WELLBY approach for demonstrating the social value of social prescribing using data collected at a national level. Wellbeing data (the study used the Office for National Statistics (ONS) Life Satisfaction measure) from more than 500 GSP participants was collected in the seven GSP sites prior to and following their engagement in nature-based activities, alongside detailed evidence about the costs associated with a full GSP pathway (i.e. the centre line in Figure 1). In the next section we provide a detailed explanation of the approach taken.
Methodology
We present the methodology for our study in two stages. First, we provide a general overview of the WELLBY approach to measuring social value, drawing on some of the extant and emergent academic literature and HM Treasury Guidance. Second, we outline how the WELLBY approach was operationalised for this study.
The WELLBY approach to measuring social value
The term WELLBY (Wellbeing Adjusted Life Year) was coined by Frijters et al. (2020) as an anthropocentric measure of social value capable of assessing progress towards the wellbeing component of the economy and steering policy decisions towards activities that create the most wellbeing (personal utility) for the financial resources invested (Frijters et al., 2024). Since then, the WELLBY has officially been adopted by HM Treasury in the UK and the New Zealand Treasury (see for example HM Treasury, 2021) as an analysis tool for both ex-ante appraisals and ex-post evaluations of public policies. WELLBYs are not limited to public policy, however. They can be used by VCSEs to demonstrate their social value to funders or by the private sector and philanthropists to track progress in relation to their Environmental, Social, and Governance (ESG) objectives.
Frijters et al. (2024) argue that a major reason for the adoption of the WELLBY by policymakers is simplicity. It utilises a single question that is included in national surveys, including the Annual Population Survey (HM Treasury, 2021), that can also be used to collect data through bespoke policy evaluation questionnaires:
Overall, how satisfied are you with your life nowadays? Give an answer on a scale of 0 to 10, where 0 is “not at all” and 10 is “completely”
This question should be easily understandable by politicians and the public and its one-dimensional measurement approach allows transparent calculations that can be replicated relatively straightforwardly. A second important reason for using WELLBYs is relevance: in the UK HM Treasury guidance (HM Treasury, 2021) states that it is most relevant when the direct aim of the policy is to improve the wellbeing of a certain group, such as through mental health programmes like the GSP project. A further important reason is overcoming complexity: the WELLBY can be especially useful for large, multi-component policy initiatives (Frijters et al., 2024) when there is evidence that wellbeing fully captures all the outcomes affected (HM Treasury, 2021).
Importantly, the WELLBY life satisfaction measure captures both hedonic and eudaimonic components of wellbeing (Díaz et al., 2015). Hedonic wellbeing focuses on experiencing positive emotions such as pleasure, and the absence of negative emotions. It is typically characterised by feeling good and enjoying life’s experiences. By contrast eudaimonic Wellbeing emphasises living a meaningful life, personal growth, and fulfilling one’s potential, typically by finding purpose and contributing to something larger than oneself.
WELLBYs can be monetised and used in social cost-benefit analyses (CBA) alongside other monetary values, or they can be used as a standalone measure of social value (Frijters et al., 2024). HM Treasury defines a WELLBY as a change in life satisfaction of one point on a scale of 0-10, per person per year, according to the Office for National Statistics (ONS) life satisfaction measure used in national surveys such as the Annual Population Survey (HM Treasury, 2021). A value of £13,000 per WELLBY is recommended (2021) with a lower estimate of £10,000 and an upper estimate of £16,000 (2019 prices). Adopting this approach enables the social value of a policy initiative to be expressed as the change in the total amount and value of WELLBYs experienced by the target population (Frijters et al., 2024) with social return on investment expressed as ratio of that value relative to the costs.
The WELLBY approach is gaining credibility in the UK, (Frijters & Krekel, 2021) with examples of its use including evaluations of the NHS Improving Access to Psychological Therapies (IAPT) programme, a nationwide mental health service to treat depression and anxiety disorders, and the 2012 London Olympics (Dolan et al., 2019). WELLBYs are also being trialled in non-governmental settings. For example, a recent study used WELLBYs to assess to the social value of Parkrun, a mass participation event based around a weekly organised five kilometre walk or run (Haake et al., 2024).
Operationalising the WELLBY approach for this study
This study takes a social return on investment (SROI) approach to expressing social value (Arvidson et al., 2013). As part of the national evaluation of the GSP project participants in nature-based activities in each of seven GSP sites were invited to participate in a monitoring questionnaire which included the ONS life satisfaction measure. Baseline measures (n=714) were collected prior to start of a nature-based intervention and post-intervention measures (n=536) were collected upon completion of the programme of activities. A total of 536 participants (75 per cent) provided pre- and post-intervention scores for life satisfaction. The time elapsed between pre- and post-intervention measures varied between activities and was dependent on the type and length of nature-based activity accessed. Most post-intervention outcome measures were collected between six weeks and 12 weeks following referral, so this range was used to derive the lower and upper WELLBY estimates.
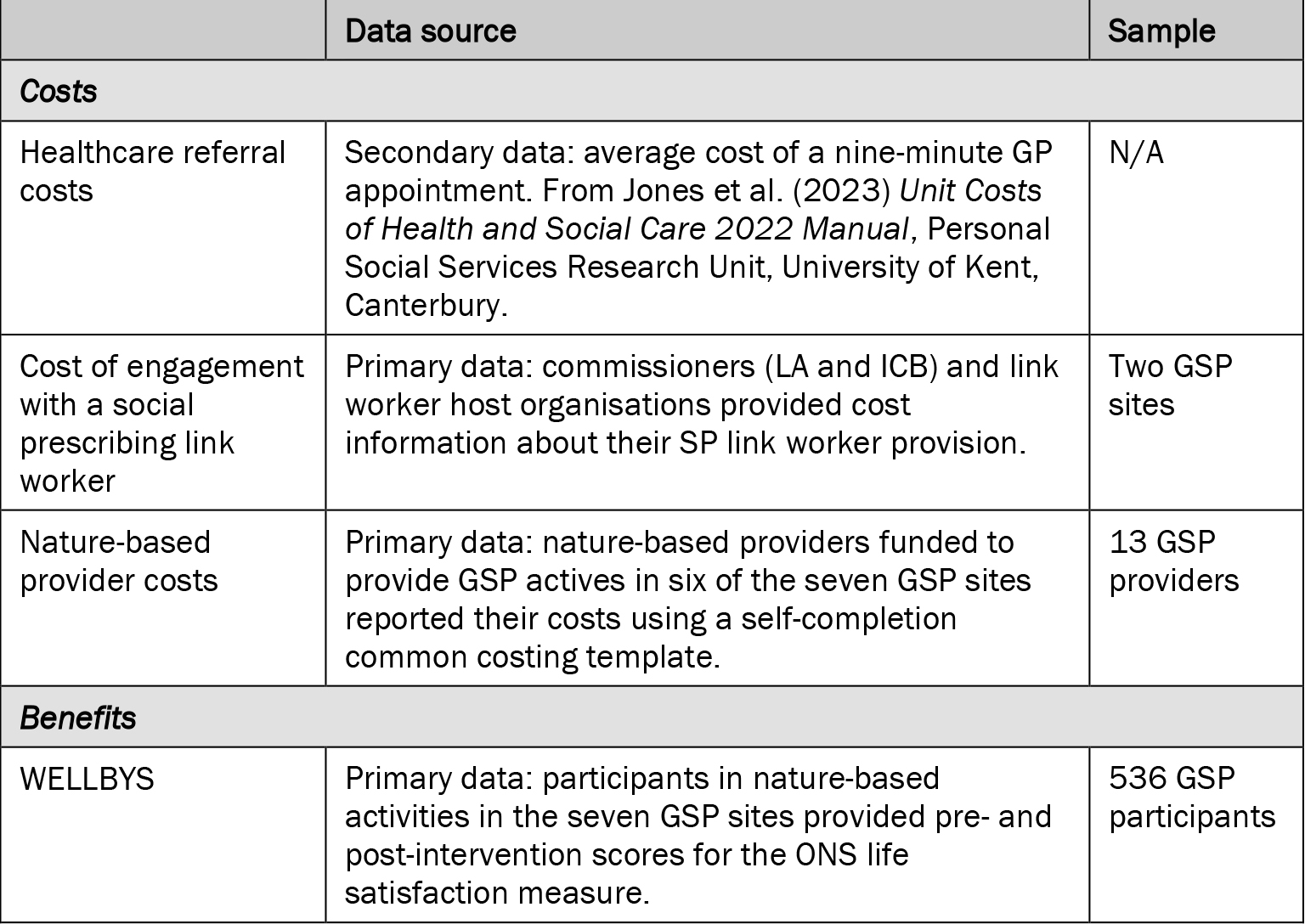
The national evaluation of the GSP project also collected data on the different costs associated with the GSP pathway presented in Figure 1. Data were derived from primary and secondary sources including national reference costs, NHS Integrated Care Boards (ICBs), local authority commissioners, link worker host organisations involved in the GSP project, and nature-based providers delivering activities funded by the GSP project. An overview of the different data sources used in this article is provided in Table 1.
Table 1: Data sources used for estimating GSP pathway costs and WELLBYs
Our approach to calculating WELLBYs involved the following stages.
- Establish costs: disaggregate GSP implementation costs and apportion to the following categories – healthcare referral, link worker engagement, nature-based provider activities.
- Calculate wellbeing gains: calculate the mean individual level change in life satisfaction scores for individuals in each site with a baseline and follow-up assessment. Confidence intervals (95 per cent) and associated p values were calculated for each of the seven sites and then at the programme level using random effects meta-analysis.
- Calculate WELLBYs:
- Estimate an annualised figure for the total number and value of WELLBYs produced per participant by multiplying the estimated mean change in life satisfaction by the WELLBY values recommended by HM Treasury.
- Calculate a prorated figure for the value of WELLBYs produced per participant based on the length of time over which outcomes were measured. This reflects HM Treasury Guidance that the value of a WELLBY should be calculated over a full year. Currently, there is no evidence about how long outcomes last, so we have not extrapolated beyond the end of nature-based activities to prevent overclaiming.
- Calculate social return on investment (SROI): divide the total value of WELLBYs created by the total costs associated with the GSP pathway.
- Sensitivity analysis: derive lower, central and upper range sensitivity estimates based on six-, nine- and 12-week outcome durations and 95 per cent confidence intervals. Develop different SROI permutations based on low, medium and high-cost nature-based activities.
The results of this process are presented sequentially in the following section.
Results
Full cost of the GSP pathway
This section presents estimates of the aggregated cost of the GSP referral pathway based on the costs associated with engagement with a healthcare professional, link worker engagement and activities provided by nature-based providers.
Cost of a referral from a healthcare professional
According to NHS reference costs the average cost of a nine-minute GP appointment is £42 (Jones et al., 2023). However, note that the referral costs of other health or social care professionals in other settings who may referral to a social prescribing link worker, will vary.
Cost of engagement with a link worker
Two GSP sites provided information about the costs and outputs associated with their social prescribing link worker provision. In site GSP01, a local VCSE organisation received funding from two primary care networks to host four full time equivalent (FTE) link workers at a total cost of £170,373 per annum (£42,593 per role). They received 1,047 referrals (pro rata) in 2022-23 making the cost per referral £163. In site GSP06, a social care department in a local authority (upper tier authority) commissioned three district councils (lower tier authorities) to host 2.6 FTE Link Workers at a total cost of £101,000 per annum (£38,846 per role). They received 697 referrals in 2021-22 making the cost per referral £145. This cost range (£145-£163) is similar to that reported in previous studies. For example, one study (Dayson & Bashir, 2014) of a VCSE social prescribing service commissioned by the NHS Clinical Commissioning Group to target people with long-term health conditions estimated that the average cost per person per year for those referred to the scheme was £188 (uprated to 2021/22 prices).
Nature-based provider activity costs
Thirteen nature-based providers from six GSP sites provided detailed data about the costs and outputs associated with their GSP provision. They were sampled purposively to provide coverage of the types of nature-based activities offered through GSP. Their work covered a broad range of nature-based activities including gardening, horticulture, physical activity, ecotherapy and animal care. Aims centred around supporting improved mental and physical health, wellbeing, and nature connection and reducing isolation and loneliness through community participation. The activities were targeted across the full spectrum of mental health needs (mild, moderate, and severe) and other complex and long-term physical and mental health conditions including PTSD, trauma, diabetes, dementia and chronic fatigue. Several providers sought to balance principles of universal access with the targeting of specific population groups or health conditions.
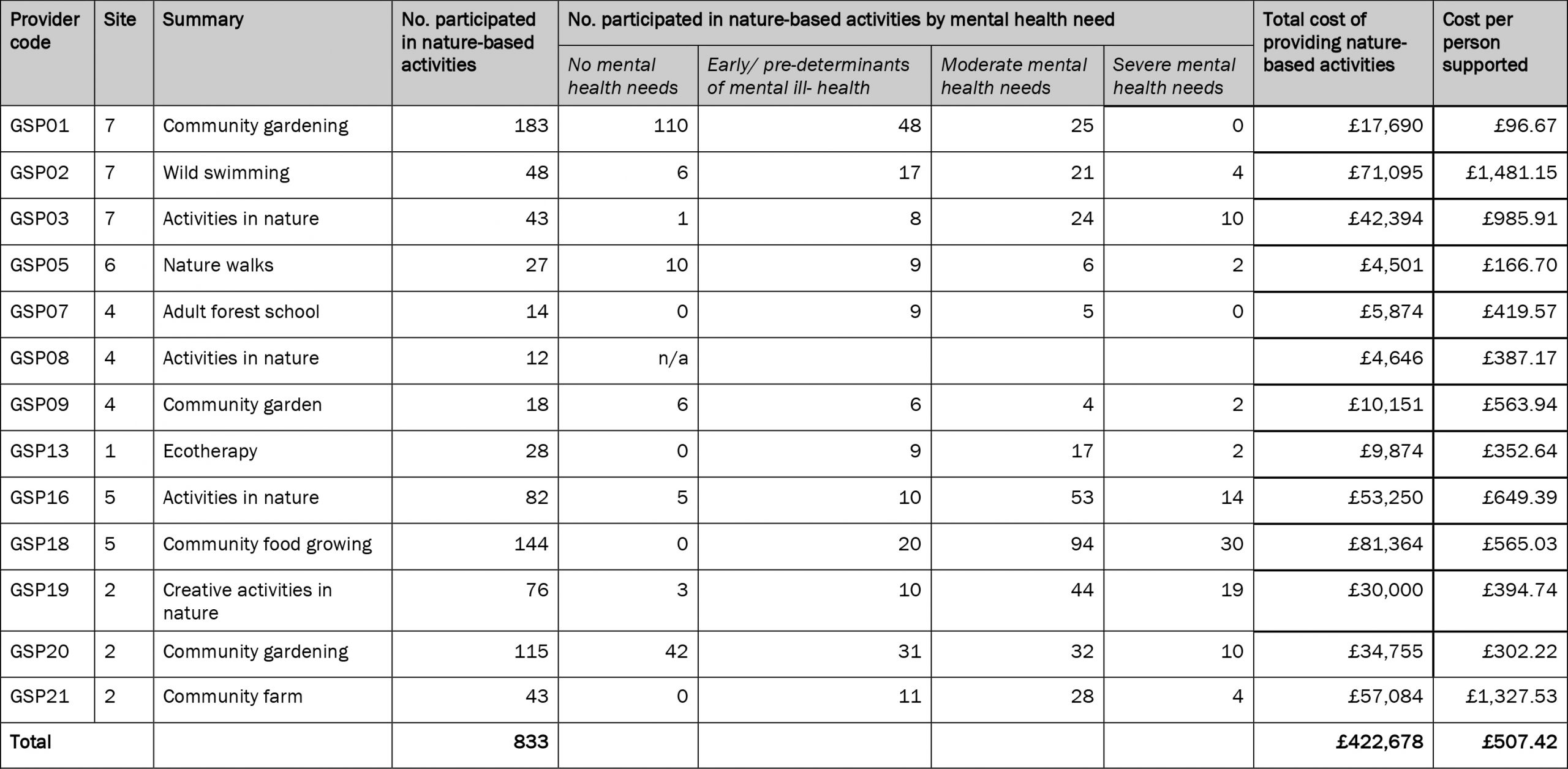
Table 2 provides an overview of the full costs and outputs of each nature-based activity to provide an estimate of the cost per person supported. This is calculated by dividing the total cost of each project by the number of people who participated in nature-based activities. Across the 13 nature-based providers, the average cost per person supported was £507.42. However, the range was very broad. GSP01 had the lowest cost per participant (£96.67), which probably reflects the high number of people accessing the activity without mental health needs. By contrast, GSP18, which had similarly high numbers of participants but far more with moderate or severe mental health needs, had a higher cost per participant (£565.03). The highest costs per participant were reported by GSP02 (£1,481.15) and GSP21 (£1,327.53). Both providers catered for a high proportion of people with moderate and severe mental health needs meaning their activities were more resource intensive to deliver in terms of staff time and the skills required. Other factors that affected the cost of provision include equipment and facilities, the duration of the intervention, the skills of the staff required to deliver the activity, and number of people it was possible to support in one session.
Table 2: Cost per participant of nature-based activities
Summarising the costs of the GSP pathway
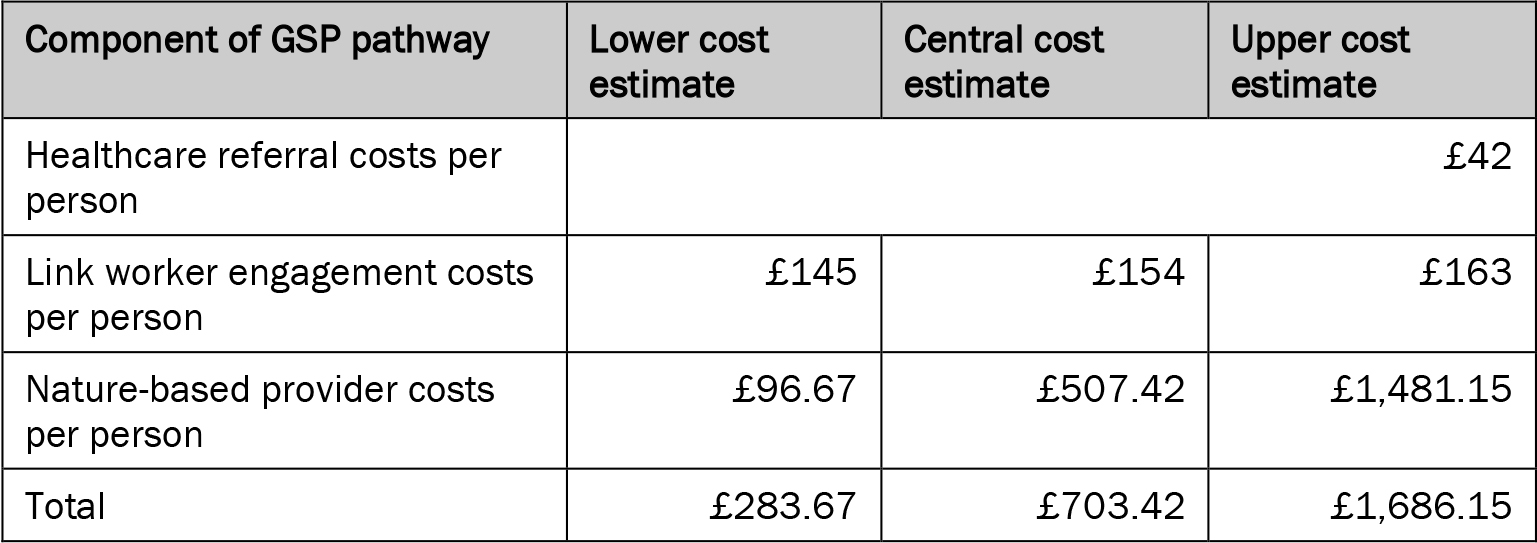
Table 3 provides an estimate of the aggregated costs associated with a GSP pathway. Based on a healthcare appointment costing £42, link worker engagement with costs ranging from £145-£163, and nature-based activity costs ranging from £96.67- £1,481.15, the overall cost of a green social pathway was estimated to be between £284-£1,686, with a mean of £703 per participant. This is a very wide range, reflecting the broad spectrum of mental health needs that these activities catered for. Nature-based activities offering universal access or catering for people with predominantly mild mental health needs tended to cost less to deliver per person than those for people with moderate and more severe needs. Supporting people with more severe needs may incur additional costs such as one-to-one support and safeguarding protocols.
Table 3: Estimate of the full cost of a GSP referral across the pathway
Estimating WELLBYs
Impact on wellbeing
There were statistically significant improvements in the wellbeing (life satisfaction) for GSP participants following engagement in nature-based activity: overall 70.4% (n=376/534) had an increase in life satisfaction score. Table 4 shows there was an increase in the average (mean) score from 4.7 to 6.8 (1.7, 95% CI: 0.7 to 2.6, p=0.001) (n=536). These means that prior to accessing GSP participants’ wellbeing was below the national average of 7.5 (Office for National Statistics, 2023) but the gap narrowed significantly after accessing GSP activities.
Table 4: Pre- and post-activity wellbeing (life satisfaction) scores for GSP participants

Base: 536 GSP participants with a pre- and post- life satisfaction score
Value of WELLBYs
The wellbeing data presented above enable WELLBYs to be calculated. Table 5 provides a range of estimates for the value of WELLBYs associated with the completion of a full GSP referral pathway. The lower estimate, based on the lower 95 per cent confidence interval (0.7-point increase in life satisfaction) and a six-week outcome duration, is £909 per referral. The middle estimate, based on the mean (1.7-point increase in life satisfaction) and a nine-week outcome period, is £4,968. The upper estimate, based on the upper 95 per cent confidence interval (2.6-point increase in life satisfaction) and a 12-week outcome period, is £10,360.
Table 5: Estimated value of WELLBYs created through completion of a full GSP referral pathway
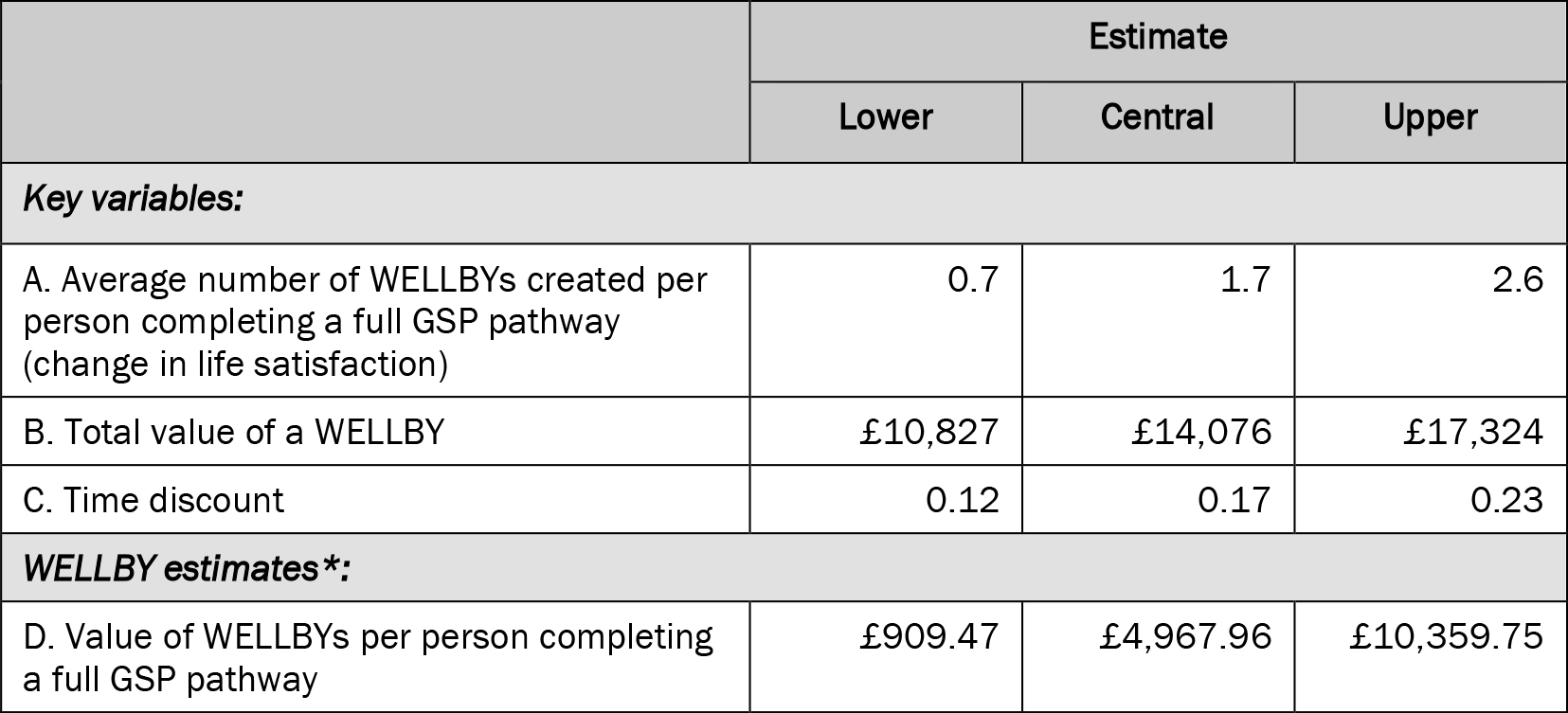
*D = (B x A) x C
Due the wide range of WELLBY values further sensitivity analysis was required to narrow these parameters. HM Treasury recommends for changes in life satisfaction greater than 0.5 points it is important to consider the impact of diminishing marginal utility of income on valuations, which is not reflected in the WELLBY approach. This is because the monetary gain associated with improvements in life satisfaction will reduce markedly for larger changes, notably changes greater than 0.5, meaning there is a risk of overestimating the number and value of WELLBYs if this is not adjusted for (HM Treasury, 2021).
In response to this guidance, we removed the central and upper range estimates for change in life satisfaction (1.7 and 2.6) in our WELLBY sensitivity estimates for GSP. Although this may oversimplify the effects of large changes in life satisfaction it mitigates the possibility of overclaiming the amount value that has been created. Revised sensitivity estimates for the number and value of WELLBYs that take this into account are provided in Table 6. The lower estimate, based on a six-week outcome duration, remains £909 per referral. The middle estimate, based on a nine-week outcome period, is £1,675. The upper estimate, based on a 12-week outcome period, is £2,789.
Table 6: Sensitivity estimate for the value of WELLBYs created through completion of a full GSP referral pathway
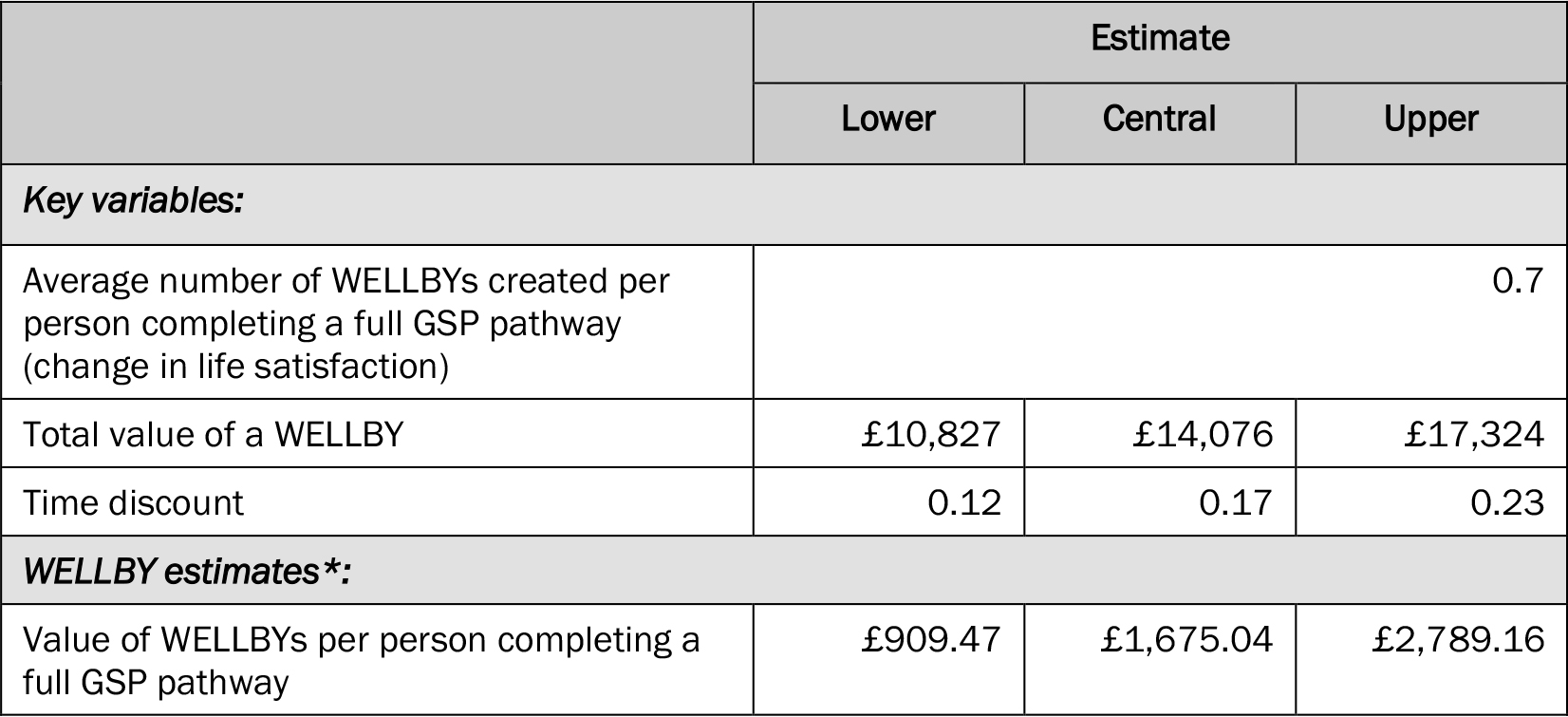
*D = (B x A) x C
Social return on Investment
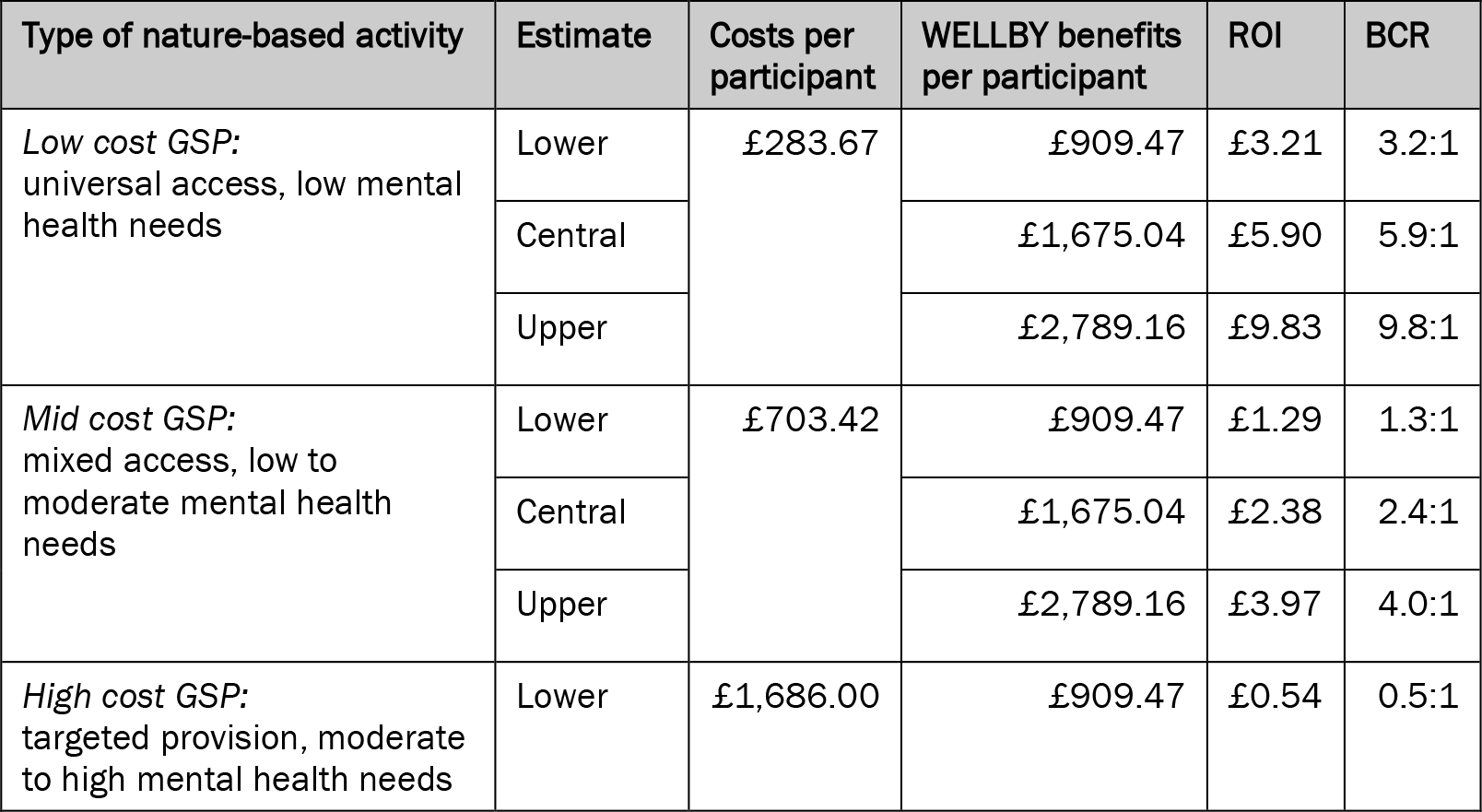
The final stage in estimating social value involves calculating the social return on investment (SROI) by dividing the value of benefits by the costs. This can also be expressed as a ratio of benefits to costs (BCR). Table 7 provides a range of estimates for the SROI/BCR of completion of a full GSP referral pathway, using WELLBYs. Lower, central and upper SROI/BCR estimates are provided for three different GSP cost permutations, drawing on the cost data presented earlier in this section. Low cost GSP, characterised by universal access for people with low mental health needs, has a SROI/BCR of between £3.21/3.2:1 and £9.83/9.9:1, with a central estimate of £5.90/5.9:1. Mid cost GSP, characterised by mixed access for people with low to moderate mental health needs, has a SROI/BCR of between £1.29/1.3:1 and £3.97/4.0:1, with a central estimate of £2.38/2.4:1. High cost GSP, characterised by targeted access for people with moderate to high mental health needs, has a SROI/BCR of between £0.34/0.3:1 and £1.65/1.7:1, with a central estimate of £0.99/1.0:1.
Table 7: Estimate of the social return on investment (SROI) of a full GSP referral pathway, using WELLBYs
Implications for policy and practice
Our results indicate that GSP can be a low-cost pathway that can lead to significant wellbeing benefits for people experiencing mental ill-health, but the costs associated with GSP vary considerably depending on who is supported and the types of nature-based activities provided. This contextual nuance is important as it affects how WELLBYs might be used to make policy and commissioning decisions. Our findings suggest that WELLBYs can be a useful social value measure for low to mid cost GSP pathways where the target participants are likely to have mild to moderate mental health needs. Our estimates show that the central SROI/BCR range for these pathways is £2.38-£5.90/2.4:1-5.9:1, indicating ‘good’ value for money. This is likely to apply to a high proportion of GSP activity which has a preventative focus. However, for higher cost pathways providing targeted support for people with more severe mental health needs, the SROI/BCR is much lower (£0.99/1.0:1) and less indicative of value for money. For these GSP pathways, which are a minority but nonetheless important component of GSP, other clinical or system focussed measures of value may be needed to demonstrate where the greatest amounts of value are being accrued.
The variation in SROI highlights an important point: GSP, like most types of social prescribing, is not one simple treatment and support pathway. In the GSP project, referrals to nature-based providers were not limited to link workers (Haywood et al, 2024). Other important sources of referral included self-referral (32 per cent), other VCSEs (eight per cent) and friends and family (seven per cent). This means that pathways to nature-based activities that do not involve a link worker, which are lower cost, could potentially offer greater value for money, as link worker costs would be excluded from the equation. Policymakers and commissioners of social prescribing and nature-based activities therefore need to consider a number of value related factors within their decision making processes: who is the intended beneficiary and what level of support will they need; what is the most appropriate referral route or routes (including whether a link worker is needed); what types of nature-based activities need to be provided (based on an understanding of the needs and preferences of the local population); and which organisations are best placed to offer these (and how should their role be resourced)?
Through our study we have identified several challenges associated with using WELLBYs to understand the social value of social prescribing projects and programmes. Overcoming these methodological, policy and practical challenges will be key to improving the utility of WELLBYs as a tool for demonstrating the social value of social prescribing in the future. Many of the challenges we have identified are methodological ones that are common to social prescribing research and research into health outcomes more generally. The first relates to data quality and quantity. For this study it was not possible to explore sub-group relationships at a granular level. For example, it would have enhanced our findings to explore wellbeing outcomes by different levels of mental health need, type of nature-based activity accessed, or level of deprivation. However, these data were either not available or collected inconsistently, limiting the amount of sub-group analysis that was possible and potentially masking variations in wellbeing outcomes for different population groups.
A second quality concern relates to the variability of the time elapsed between pre- and post-intervention wellbeing measures due to differences in the type and length of nature-based activities. As discussed, most post-intervention outcome measures were collected between six weeks and 12 weeks following referral, meaning it was not possible to measure WELLBYs over a full year. Future studies should consider extending their post-intervention outcome measurement point to at least six or 12 months to enable analysis of longer-term benefits. It may be that the initial wellbeing gains are sustained, but they may reduce or increase depending on individual behaviours and factors outside of their involvement in GSP or nature-based activities.
A third quality concern relates to the absence of a control or comparator group within our wellbeing data. Establishing and collecting data from a geographic area or population group with access to GSP and/or nature-based activities was beyond the scope of the GSP project and its evaluation. This means that we do not know the extent to which the improvements in wellbeing would have occurred without participating in nature-based activities or the influence of other activities or interventions. As such, it was not possible to establish deadweight or the additionality of the wellbeing outcomes observed, meaning a value for net additional WELLBYs has not been estimated. Given the universality of link worker provision, the ambition to spread and scale GSP nationally in future years, and the complexity associated with GSP, a large randomised controlled trial (RCT) of the whole GSP pathway is likely to be infeasible. In future national studies it may be possible to derive a synthetic matched sample using national wellbeing data, for example from the Annual Population Survey, but further methodological development would first be required.
There are also some policy related challenges associated with using WELLBYs to demonstrate the value of social prescribing. These challenges concern how wellbeing evidence such as WELLBYs can be used to inform decisions about which services are commissioned and how public sector resources are allocated, locally and nationally. Although WELLBYs are endorsed by HM Treasury in the UK, and despite growing global interest in their utility as a policy tool, it is not clear that all policy makers currently possess the knowledge, skills and understanding to use the evidence in practice. The GSP project provides an illustration of this. Feedback from national policymakers (including HM Treasury) indicated that the WELLBY evidence was not sufficient to make a business case for future investment in GSP and that further evidence about system benefits (i.e. relieving pressure on health systems) was required. By contrast, at a local level, some GSP sites have reported using the WELLBY evidence to generate business cases for further investment in nature-based activities, and this had been received positively by local decision makers within the health system. In one GSP site an additional £200,000 was allocated by the NHS to fund nature-based providers due to the positive WELLBY evidence that was presented.
A final set of challenges relate to the practicalities of collecting wellbeing data for link workers and VCSE providers operating in nature-based settings. These were identified through the wider GSP project evaluation (see Haywood et al, 2024). Although the ONS wellbeing question from which WELLBYs can be calculated is mandated by the NHS for all link workers, they receive very little training about how to collect the data, have limited guidance about why it is important, and struggle to access patient-level or aggregate data once it has been recorded. Unsurprisingly, this leads to low levels of buy-in and concerns about data completeness and quality. Similarly, nature-based VCSE providers rarely receive training about how to collect wellbeing data or feedback about how the data has been used. VCSE providers also report challenges in convincing participants to complete the required questionnaires and argue their implementation can be counter to their wider ethos, aims and processes. Participants can put be off by the wording, which may reintroduce unwelcoming feelings and lead to re-traumatisation, and questionnaires can be difficult to implement practically in nature-based settings.
Conclusion
This article has presented national level findings about the social value of social prescribing using the WELLBY approach. The findings indicate that this approach can be most effectively used to measure the social value of low to mid cost GSP pathways where the target beneficiaries are likely to have mild to moderate mental health needs. In these contexts, the WELLBY approach has three main advantages over other approaches that tend to be used to measure the value of social prescribing. First, it offers a potentially more relevant person-centred counterpoint to approaches that are more clinical health system centric. Second, it provides a more consistent and simple approach to measuring personal and societal benefits than other SROI approaches. Third, it offers the potential to measure benefits at a national and international level, including drawing on large datasets of routinely collected measures such as the ONS life satisfaction question. For these advantages to be realised, our findings suggest that a number challenges relating to how WELLBY evidence is collected, analysed and used by policy makers need to be overcome.
Although not explored explicitly in our study, it is also important to consider what the limitations of the WELLBY approach might be. We should consider what such a simple and one-dimensional measure could mask or subvert in relation to individual experiences, outcomes and attributes, and how participants from different backgrounds may experience an intervention and wellbeing differently. The WELLBY should not be adopted uncritically, and those using it to inform decision making should consider what other types of evidence may be useful as well. Looking beyond social prescribing, WELLBYs hold some promise for policymakers seeking to understanding the benefits of other similar community-based VCSE-led activities and services. If used appropriately WELLBYs could be useful to health systems and other public bodies seeking to understand the broader benefits of their investments in the VCSE sector, particularly where these are likely to be preventative and address inequalities, rather than produce direct or immediate clinical or system level benefits.
This article has been developed by a team of researchers commissioned by Defra to undertake an independent evaluation of the Preventing and Tackling Mental Ill Health through Green Social Prescribing Project (2021-23). The main evaluation report referenced throughout this article, and the accompanying briefing, summary and appendices documents, are published by Defra (Defra Project Code BE0191) and are available from the Department’s Science and Research Projects Database at https://randd.defra.gov.uk
Whilst the research was commissioned by Defra, the views expressed in this article reflect the evaluation findings and the authors’ subsequent analysis of the data; they do not necessarily reflect Defra policy.
Chris Dayson. Email: c.dayson@shu.ac.uk
Arvidson, M., Lyon, F., McKay, S., & Moro, D. (2013). Valuing the social? The nature and controversies of measuring social return on investment (SROI). Voluntary sector review, 4(1), 3-18. CrossRef link
Beiderbeck, D., Frevel, N., van derGracht, H., Schmidt, S., & Schweitzer, V. (2021). Preparing, conducting, and analyzing Delphi surveys: Cross-disciplinary practices, new directions, and advancements. MethodsX, 8, 101401. CrossRef link
Canadian Red Cross (2024). A Healthier Canada. An Analysis of the Potential Economic and Social Impacts of Social Prescribing. https://irp.cdn-website.com/92bb31b3/files/uploaded/A_Healthier_Canada-An_Analysis_of_the_Potential_Economic_and_Social_Impacts_of_Social_Prescribing.pdf
Bertotti, M., Frostick, C., & Temirov, O. (2020). An evaluation of Social Prescribing in the London Borough of Redbridge: final evaluation report. London Borough of Redbridge and the Redbridge Clinical Commissioning Group, Health and Well-being Fund
Dayson, C. (2017). Policy commentary – Social prescribing “plus”: a model of asset-based collaborative innovation? People Place Policy, 11(2), 90-104. CrossRef link
Dayson, C., & Bashir, N. (2014). The social and economic impact of the Rotherham Social Prescribing Pilot: Main evaluation report. Sheffield Hallam University. https://www.shu.ac.uk/centre-regional-economic-social-research/publications/the-social-and-economic-impact-of-the-rotherham-social-prescribing-pilot-main-evaluation-report
Dayson, C., Painter, J., & Bennett, E. (2020). Social prescribing for patients of secondary mental health services: emotional, psychological and social wellbeing outcomes. Journal of Public Mental Health, 19(4), 271-279. CrossRef link
Díaz, D., Stavraki, M., Blanco, A., & Gandarillas, B. (2015). The eudaimonic component of satisfaction with life and psychological well-being in Spanish cultures. Psicothema, 27(3), pp 247-53. CrossRef link
Dolan, P., Kavetsos, G., Krekel, C., Mavridis, D., Metcalfe, R., Senik, C., Szymanski, S., & Ziebarth, NR, (2019). Quantifying the intangible impact of the Olympics using subjective well-being data. Journal of Public Economics, 177, 104043, CrossRef link
de Bell, S., Alejandre, J., Menzel, C., Sousa-Silva, R., Straka, T., Berzborn, S., Bürck-Gemassmer, M., Dallimer, M., Dayson, C., Fisher, J., Haywood, A., Herrmann, A., Immich, G., Keßler, C., Köhler, K., Lynch, M., Marx, V., Michalsen, A., Mudu, P., Napierala, H., Nawrath, M., Pfleger, S., Quitmann, C., Reeves, J., Rozario, K., Straff, W., Walter, K., Wendelboe-Nelson, C., Marselle, M., Oh, R., & Bonn, A. (2024). Nature-based social prescribing programmes: opportunities, challenges, and facilitators for implementation. Environment International, 190, CrossRef link
Frijters, P., Clark, A.E., Krekel, C., & Layard, R. (2020). A happy choice: wellbeing as the goal of government. Behavioural Public Policy, 4(2),126-165. CrossRef link
Frijters, P, & Krekel, C. (2021). A handbook for wellbeing policy-making. Oxford University Press. CrossRef link
Frijters, P., Krekel, C., Sanchis, R. & Santini, Z.. (2024). The WELLBY: a new measure of social value and progress. Humanities and Social Sciences Communications, 11, 736. CrossRef link
Foster, A., Thompson, J., Holding, E., Ariss, S., Mukuria, C., Jacques, R., Akparido, R., & Haywood, A. (2021). Impact of social prescribing to address loneliness: A mixed methods evaluation of a national social prescribing programme. Health and Social Care in the Community, 29, 1439-1449. CrossRef link
Fullam, J., Hunt, H., Lovell, R., Husk, K., Byng, R., Richards, D., Bloomfield, D., Warber, S., Tarrant, M., Lloyd, J., Orr, N., Burns, L., & Garside, T. (2021). A handbook for Nature on Prescription to promote mental health. Version 1. University of Exeter.
Haake, S., Quirk, H., & Bullas, A. (2024). The impact of parkrun on life satisfaction and its cost-effectiveness: A six-month study of parkrunners in the United Kingdom. PLOS Global Public Health, 4(10), e0003580. CrossRef link
Hayes, D., Olsson, A., Begum, S., Bertotti, M., Jarvis-Beesley, P., & Stapley, E. (2024). Barriers and facilitators to social prescribing in child and youth mental health: perspectives from the frontline. European Child & Adolescent Psychiatry, 33, 1465-1479. CrossRef link
Haywood, A., Dayson, C., Garside, R., Foster, A., Lovell, R., Husk, K., Holding, E., Thompson, J., Shearn, K., Hunt, H.A., Dobson, J., Harris, C., Jacques, R., Witherley, D., Northall, P., Baumann, M., & Wilson, I. (2024). National Evaluation of the Preventing and Tackling Mental Ill Health through Green Social Prescribing Project: Final Report. Department for Environment, Food and Rural Affairs.
HM Treasury (2021). Wellbeing Guidance for Appraisal: Supplementary Green Book Guidance.
Husk, K., Blockley, K., Lovell, R., Bethel, A., Lang, I., Byng, R., & Garside, R. (2020). What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health and Social Care in the Community, 28, 309–324. CrossRef link
Husk, K., & Sanderson, J. (2024). Social Prescribing in England. In: Bertotti, M. (eds) Social Prescribing Policy, Research and Practice. Springer. CrossRef link
Jones, K., Weatherly, H., Birch, S., Castelli, A., Chalkley, M., Dargan, A., Forder, J., Gao, M., Hinde, S., Markham, S., Ogunleye, D., Premji, S., & Roland, D. (2023). Unit Costs of Health and Social Care 2022 Manual, Personal Social Services Research Unit, University of Kent.
Jones, K. & Burns, A. (2021). Unit Costs of Health and Social Care 2021, Personal Social Services Research Unit, University of Kent.
Kimberlee, R. (2016). What is the value of social prescribing? Advances in Social Sciences Research Journal, 3(3). pp. 29-35. CrossRef link
Morse, D., Sandhu, S., Mulligan, K., Tierney, S., Polley, M., Chiva Giurca, B., Slade, S., Dias, S., Mahtani, K., Wells, L., Wang, H., Zhao, B., De Figueiredo, C., Joost Meijs, J., Kweun Nam, H., Lee, K H., Wallace, C., Elliott, M., Mendive, J.M., Robinson, D., Palo, M., Herrmann, W., Østergaard Nielsen, R., & Husk, K. (2022). Global developments in social prescribing. BMJ Global Health, 7, e008524. CrossRef link
Muhl, C., Mulligan, K., Bayoumi, I., Ashcroft, R., & Godfrey, C. (2023). Establishing internationally accepted conceptual and operational definitions of social prescribing through expert consensus: a Delphi study. BMJ Open, 13, e070184. CrossRef link
National Academy for Social Prescribing (2024). Social Prescribing Around the World – A World Map of Global Developments in Social Prescribing Across Different Health System Contexts: 2024
NHS (2019). The NHS Long Term Plan. Department for Health and Social Care; 2019. https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf
O’Connell Francischetto, E. (2024). The impact of social prescribing on health service use and costs: Examples of local evaluations in practice. National Academy for Social Prescribing.
Office for National Statistics. (2023, November 7). Personal well-being in the UK: April 2022 to March 2023. https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/bulletins/personalwellbeingintheuk/april2022tomarch2023
Polley, M., Whitehouse, J., Elnaschie, S., & Fixsen, A. (2019). What does successful social prescribing look like – mapping meaningful outcomes. University of Westminster.